Prednisone, a corticosteroid, frequently serves as a first-line treatment for autoimmune hemolytic anemia (AIHA). Its mechanism involves suppressing the immune system’s excessive destruction of red blood cells, thereby improving anemia symptoms. Expect improvements in fatigue, pallor, and shortness of breath within weeks of starting treatment, though the timeline varies significantly among patients.
Dosage typically starts at 1 mg/kg per day, adjusted based on your response and potential side effects. Common side effects include weight gain, increased appetite, fluid retention, and mood changes. Regular blood tests monitor your response to treatment, guiding necessary dosage adjustments. Closely monitor your blood pressure and blood sugar levels during treatment.
While Prednisone often provides relief, long-term use carries risks. Weaning off Prednisone is a gradual process, typically over several months, to minimize relapse. Your doctor will create a personalized tapering schedule, carefully reducing the dose incrementally. Alternative treatments, such as rituximab or splenectomy, may be considered if Prednisone proves insufficient or if side effects are intolerable.
Remember: This information provides general guidance. Always consult your physician for personalized treatment plans and to address any specific concerns. Open communication with your healthcare team is critical for successful management of AIHA.
- Autoimmune Hemolytic Anemia and Prednisone
- Understanding Autoimmune Hemolytic Anemia (AIHA)
- Prednisone’s Mechanism of Action in AIHA
- Impact on Cytokines and Inflammation
- Dosage Considerations and Monitoring
- Typical Prednisone Dosage and Administration for AIHA
- Dosage Adjustments
- Maintenance Therapy and Alternative Approaches
- Monitoring Response to Prednisone Treatment
- Frequency of Blood Tests
- Other Important Indicators
- Reporting Symptoms
- Long-Term Monitoring
- Potential Side Effects of Prednisone in AIHA Treatment
- Alternative Treatments When Prednisone Fails
- Second-Line Treatment Options
- Blood Transfusions
- Long-Term Management and Relapse Prevention
- Alternative Therapies and Second-Line Treatments
- Lifestyle Adjustments
Autoimmune Hemolytic Anemia and Prednisone
Prednisone, a corticosteroid, commonly treats autoimmune hemolytic anemia (AIHA) by suppressing the immune system’s attack on red blood cells. Your doctor will determine the appropriate dosage based on your specific condition and response to treatment. Typical starting doses range from 1 to 2 milligrams per kilogram of body weight daily, but this can vary significantly.
Expect potential side effects, including weight gain, fluid retention, increased appetite, mood changes, and increased risk of infection. Regular monitoring of blood counts and overall health is crucial while taking prednisone. Your physician will adjust the dosage based on your progress. A slow tapering of the dose is necessary to minimize withdrawal symptoms once remission is achieved, preventing a relapse.
Alternative treatments may be considered if prednisone proves ineffective or causes intolerable side effects. These might include other immunosuppressants like rituximab or azathioprine, or even splenectomy in severe cases. Your healthcare provider will discuss these options with you.
| Possible Side Effects of Prednisone | Management Strategies |
|---|---|
| Weight gain | Diet modifications, exercise |
| Fluid retention | Dietary sodium restriction |
| Increased appetite | Mindful eating habits |
| Mood changes | Open communication with your doctor |
| Increased risk of infection | Practice good hygiene, avoid crowds |
Close collaboration with your hematologist is vital for managing AIHA and optimizing your prednisone treatment. Regular follow-up appointments ensure monitoring and timely adjustments to your therapy plan. Open communication regarding any concerns or side effects is key to achieving the best possible outcome.
Understanding Autoimmune Hemolytic Anemia (AIHA)
Autoimmune hemolytic anemia (AIHA) occurs when your immune system mistakenly attacks and destroys your own red blood cells. This leads to anemia, characterized by fatigue, weakness, and shortness of breath.
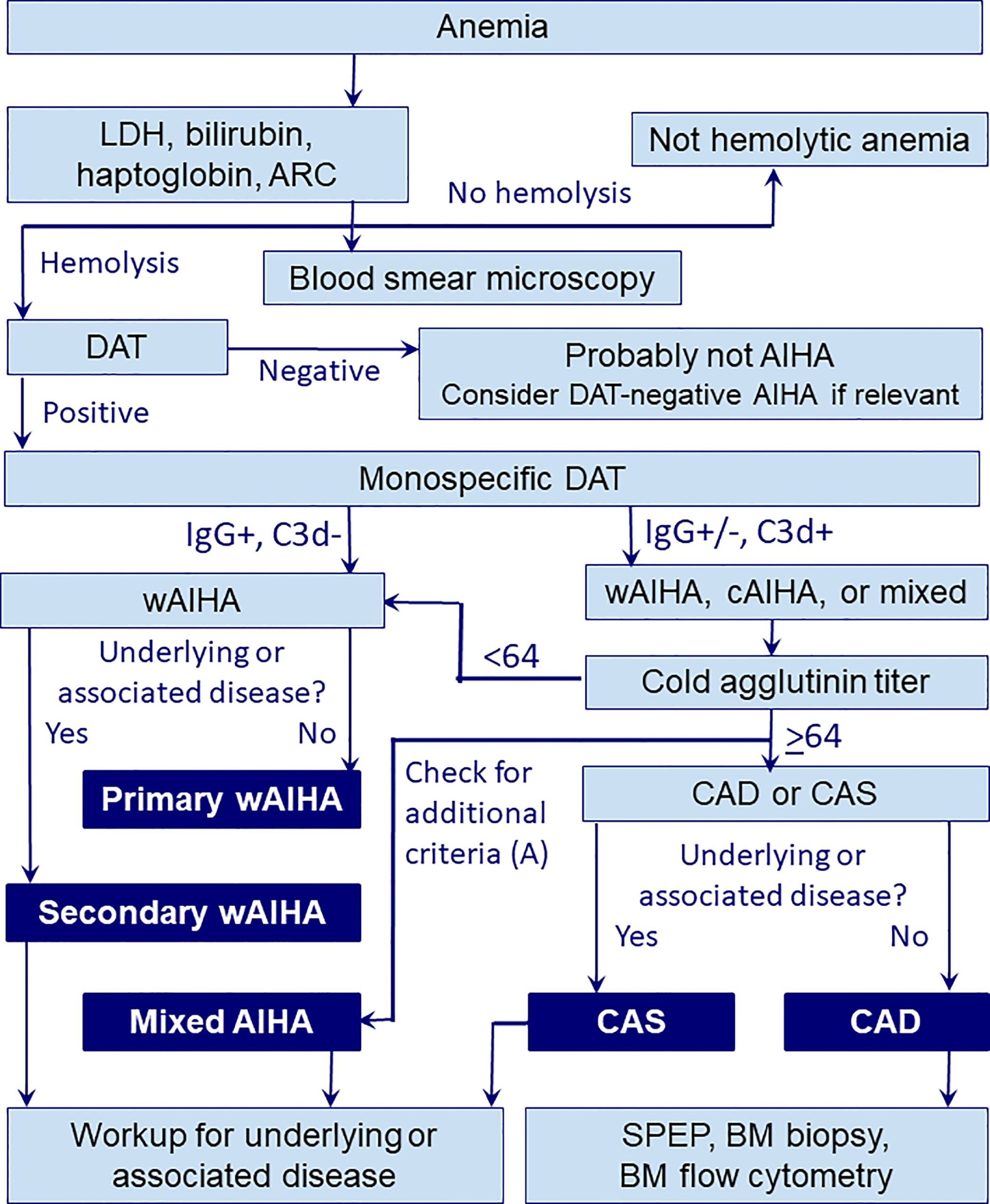
Several types of AIHA exist, categorized by the type of antibody involved and the temperature at which the antibody reacts best:
- Warm antibody AIHA: The most common type; antibodies react best at normal body temperature.
- Cold antibody AIHA: Antibodies react best at lower temperatures; often associated with infections like Mycoplasma pneumoniae.
- Mixed-type AIHA: Features characteristics of both warm and cold antibody AIHA.
AIHA diagnosis relies on several tests:
- Complete blood count (CBC): Shows reduced red blood cell count, hemoglobin, and hematocrit.
- Peripheral blood smear: Examines red blood cell shape and size for abnormalities, such as spherocytes (small, round red blood cells).
- Direct antiglobulin test (DAT) or Coombs test: Detects antibodies attached to red blood cells.
- Indirect antiglobulin test (IAT): Detects antibodies in the blood serum.
Treatment depends on the severity of the anemia and the underlying cause. Options include:
- Corticosteroids (like prednisone): Suppress the immune system, reducing red blood cell destruction. Dosage and duration vary greatly.
- Immunosuppressive drugs: Used if corticosteroids are ineffective or cause unacceptable side effects.
- Splenectomy: Surgical removal of the spleen, which plays a role in red blood cell destruction.
- Intravenous immunoglobulin (IVIG): Provides temporary immune system modulation.
- Rituximab: A targeted therapy reducing B-cells involved in antibody production.
Regular monitoring of blood counts and careful management of symptoms are critical for long-term health. Always consult your physician for appropriate diagnosis and treatment. Self-treating is dangerous and can lead to complications.
Prednisone’s Mechanism of Action in AIHA
Prednisone, a glucocorticoid, suppresses the immune system in autoimmune hemolytic anemia (AIHA) through several key mechanisms. It reduces the production of autoantibodies by directly inhibiting B-cell activation and proliferation. This decrease in autoantibody production leads to a lower rate of red blood cell destruction. Furthermore, prednisone dampens the activity of macrophages, the immune cells responsible for engulfing and destroying antibody-coated red blood cells. This reduces red blood cell destruction, improving anemia symptoms.
Impact on Cytokines and Inflammation
Prednisone also influences the production of pro-inflammatory cytokines, such as TNF-α and IL-1, which contribute to the inflammation underlying AIHA. By decreasing cytokine production, prednisone mitigates the inflammatory response, leading to reduced hemolysis. This anti-inflammatory effect helps to improve the overall clinical picture.
Dosage Considerations and Monitoring
The precise dosage of prednisone and the treatment duration are tailored to the individual patient’s response and disease severity. Regular blood tests, including complete blood counts and reticulocyte counts, are crucial for monitoring the effectiveness of the treatment and adjusting the dosage as needed. Close monitoring allows for early detection of potential side effects, enabling timely intervention.
Typical Prednisone Dosage and Administration for AIHA
Initial treatment usually begins with a high dose of prednisone, often 1 to 1.5 mg/kg per day orally. This high dose is typically administered in divided doses throughout the day for better absorption and to minimize side effects. For example, a 70kg individual might receive 70-105mg daily, divided into three or four doses.
Dosage Adjustments
Doctors closely monitor blood counts (hemoglobin and reticulocytes) to gauge treatment response. If the response is satisfactory, the prednisone dose is gradually reduced over several weeks or months. This tapering process aims to maintain remission while minimizing long-term steroid side effects. The reduction schedule is highly individualized, based on the patient’s response. A typical approach might involve decreasing the dose by 5-10mg every few days or weeks.
Maintenance Therapy and Alternative Approaches
Once remission is achieved, many patients require a low maintenance dose of prednisone for several months to prevent relapse. Some individuals might require longer periods of maintenance therapy, potentially years, while others may achieve complete remission without ongoing steroid use. If prednisone is ineffective or causes intolerable side effects, alternative therapies, such as rituximab or splenectomy, might be considered.
Monitoring Response to Prednisone Treatment
Regular blood tests are key. Expect your doctor to monitor your complete blood count (CBC), specifically hemoglobin and hematocrit levels, weekly or bi-weekly initially. These tests measure the number of red blood cells and the amount of hemoglobin in your blood, directly indicating the effectiveness of prednisone in boosting red blood cell production.
Frequency of Blood Tests
The frequency of blood tests will adjust based on your response. As your hemoglobin and hematocrit levels improve and stabilize, the interval between tests might increase to monthly or even less frequent checkups. Your physician will adjust this schedule according to your individual progress.
Other Important Indicators
Beyond CBC, your doctor may also order reticulocyte counts. Reticulocytes are immature red blood cells, and an increase in their number shows your bone marrow is responding to the treatment and producing new red blood cells. Monitoring these values provides a more detailed picture of your bone marrow’s activity.
Reporting Symptoms
Active communication is crucial. Report any persistent symptoms, even seemingly minor ones, to your physician. Fatigue, shortness of breath, or jaundice could indicate the prednisone isn’t working effectively or that complications have arisen. Your doctor needs this information to tailor your treatment plan.
Long-Term Monitoring
Long-term monitoring is essential even after your symptoms improve. The goal is to find the lowest effective prednisone dose to minimize side effects while maintaining disease control. This often involves gradual dose reduction under close medical supervision, with continued blood tests to track your response. Regular appointments and open communication with your healthcare team are necessary for successful management of autoimmune hemolytic anemia.
Potential Side Effects of Prednisone in AIHA Treatment
Prednisone, while highly effective in managing Autoimmune Hemolytic Anemia (AIHA), carries potential side effects. Understand these to better manage your treatment.
Weight gain is common due to fluid retention and increased appetite. Maintain a healthy diet and regular exercise to mitigate this. Your doctor can also discuss strategies for weight management.
Increased blood sugar is another possibility, particularly in individuals predisposed to diabetes. Regular blood glucose monitoring is vital. Your physician might adjust your medication or recommend lifestyle changes.
Mood swings, ranging from irritability to anxiety or depression, can occur. Open communication with your doctor is crucial; they may suggest counseling or adjust your Prednisone dosage.
Increased risk of infection is a serious consideration. Practice good hygiene and report any signs of infection immediately. Your immune system is suppressed while on Prednisone.
Osteoporosis is a long-term risk with prolonged Prednisone use. Maintain adequate calcium and vitamin D intake, and discuss bone density testing with your doctor.
High blood pressure can develop. Regular blood pressure checks are necessary. Your doctor might prescribe additional medication to manage this.
Gastrointestinal issues, such as heartburn, nausea, or ulcers, can arise. Follow your doctor’s advice on taking Prednisone with food and report any stomach problems.
Muscle weakness and thinning of the skin are also possible. A balanced diet and gentle exercise can help manage these side effects.
Remember, these are potential side effects; not everyone experiences them. Regular monitoring and open communication with your healthcare provider are key to managing these risks and ensuring successful AIHA treatment.
Alternative Treatments When Prednisone Fails
If prednisone isn’t controlling your autoimmune hemolytic anemia, your doctor will likely explore other treatment options. These might include:
- Rituximab: This monoclonal antibody targets B cells, reducing antibody production that damages red blood cells. Expect regular blood tests to monitor its effects.
- Other immunosuppressants: Drugs like azathioprine, mycophenolate mofetil, or cyclosporine can suppress your immune system, lessening red blood cell destruction. These medications require close monitoring for side effects.
- Splenectomy: Surgical removal of the spleen, a major site of red blood cell destruction, can significantly improve symptoms in some patients. Post-surgery, you’ll need vaccinations to prevent infections.
Second-Line Treatment Options
Should initial treatments prove insufficient, your physician might consider:
- Immunoglobulin therapy: Intravenous immunoglobulin (IVIg) can temporarily suppress the immune system and improve red blood cell survival. It’s often used for short-term management or during flare-ups.
- Eculizumab: This targeted therapy inhibits a protein crucial in complement activation, a key process in autoimmune hemolytic anemia. It is typically reserved for severe cases. Careful monitoring for infections is crucial.
- Corticosteroids with other immunosuppressants: Combining prednisone with other immunosuppressants can enhance efficacy. This combination often reduces the dose of prednisone required.
Blood Transfusions
Regular blood transfusions may be needed to maintain adequate hemoglobin levels while other treatments are initiated or take effect. While transfusions address immediate needs, they don’t treat the underlying cause of your anemia.
Remember: Treatment plans are individualized. Discuss all options thoroughly with your hematologist to find the best approach for your specific situation and health needs. Close monitoring and regular follow-up are always essential parts of managing autoimmune hemolytic anemia.
Long-Term Management and Relapse Prevention
Maintain close contact with your hematologist. Regular blood tests, including complete blood counts (CBCs) and reticulocyte counts, monitor your response to treatment and detect early signs of relapse. Adjusting prednisone dosage or exploring alternative therapies becomes easier with frequent monitoring.
Consider using lower doses of prednisone for maintenance therapy if your disease is under control. This reduces the risk of long-term side effects. Your doctor will help you determine the best maintenance dose for you. This may include a slow tapering of the prednisone dose over several months. Always follow your doctor’s instructions.
Alternative Therapies and Second-Line Treatments
If prednisone alone isn’t sufficient, your doctor may suggest other immunosuppressants, such as azathioprine, mycophenolate mofetil, or rituximab. These medications can help to suppress the immune system and reduce the production of autoantibodies. Discuss potential benefits and side effects of each option with your physician to make an informed choice.
Lifestyle Adjustments
While not a cure, maintaining a healthy lifestyle can support your overall well-being and potentially reduce relapse frequency. Focus on a balanced diet, regular exercise, and sufficient rest. Manage stress effectively through techniques like meditation or yoga. Minimize exposure to potential infections, as these can trigger flares. Promptly address any illnesses or infections with appropriate medical attention.
Participating in support groups or online communities can provide emotional support and a platform to share experiences with others living with autoimmune hemolytic anemia. This can greatly enhance your coping mechanisms and overall quality of life.